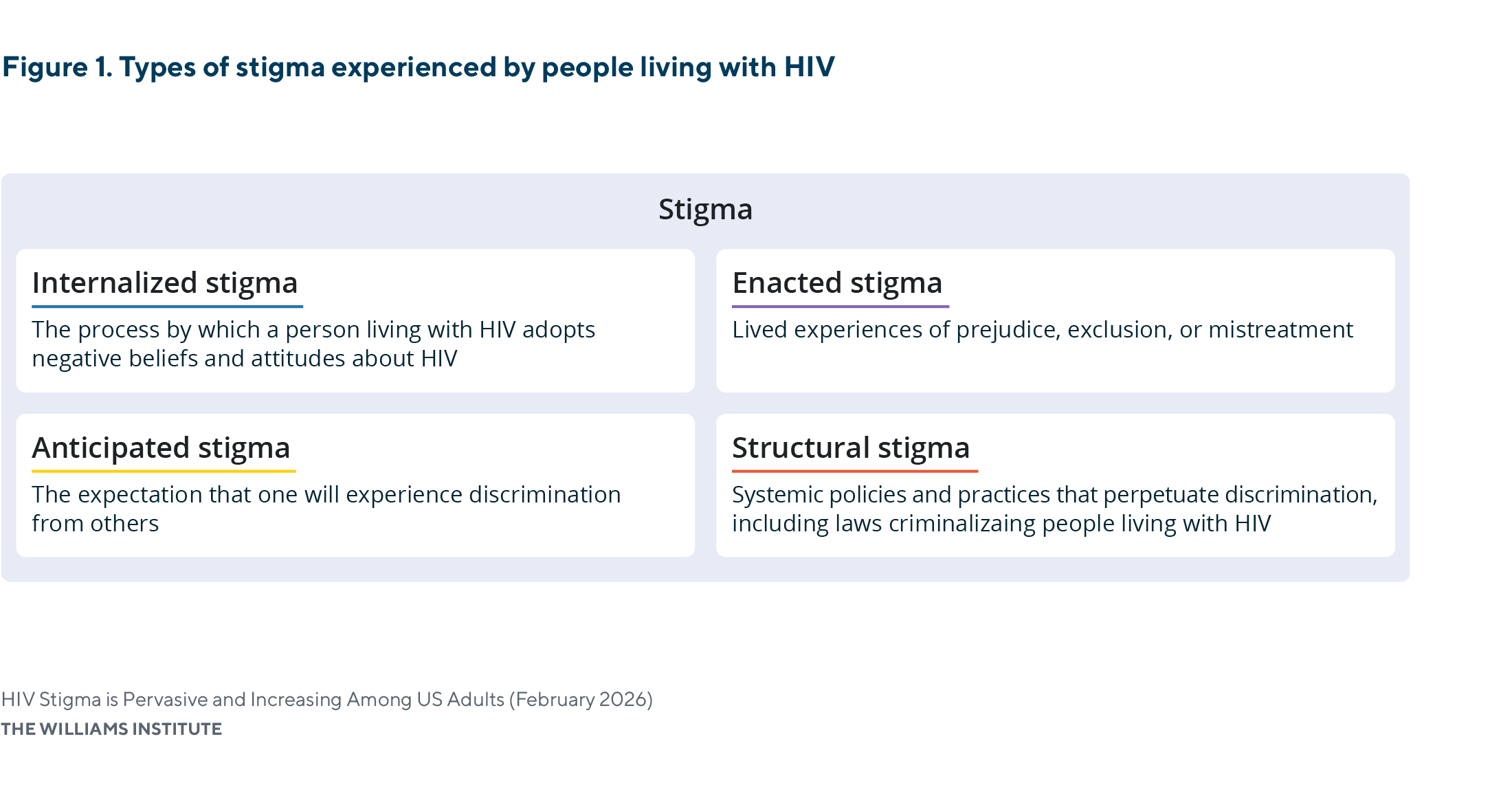
HIV stigma remains a persistent challenge shaping responses to the HIV epidemic in the United States. For people living with HIV (PLWH), stigma can directly affect health and well-being, including poorer mental health outcomes, reduced engagement in care, and lower quality of life. Stigma also adversely affects physical health outcomes by decreasing HIV testing, engagement in care, and treatment adherence, limiting achievement of an undetectable viral load, and increasing the risk of transmission. Stigma manifests through internalized stigma, referring to the internal adoption of negative beliefs about HIV; anticipated stigma, or expectations of discrimination from others; enacted stigma, which involves actual experiences of prejudice, exclusion, or mistreatment; and structural stigma, which refers to the policies, laws, and institutional practices that systemically disadvantage PLWH.
HIV Stigma is Pervasive and Increasing Among US Adults
This study uses data from the nationally representative General Social Survey to assess the prevalence of HIV stigma in the U.S. and examine the ways HIV stigma contributes to the criminalization of people living with HIV.
Scientific evidence demonstrates that, when viewed as a medical issue and with consistent antiretroviral therapy, HIV is a manageable chronic condition. Individuals with sustained viral suppression—achieved through medication to undetectable levels—do not transmit HIV sexually. Despite this evidence, HIV stigma persists and operates through fear-based beliefs, exaggerated perceptions of transmission risk, and negative attitudes toward PLWH. These misperceptions, including moral judgements and medically inaccurate beliefs that PLWH pose a threat to others, continue to shape public attitudes toward HIV. At a broader level, individual beliefs contribute to structural forms of HIV stigma, including policies, public health practices, and legal frameworks that discriminate against PLWH based on the basis of their medical status. Structural HIV stigma has, in turn, been linked to inequities in access to housing, employment, and health care for PLWH.
One manifestation of structural HIV stigma is HIV criminalization, which refers to criminal laws that punish people because of their HIV-positive status or that impose enhanced criminal penalties on the basis of a person’s HIV-positive status. Many HIV criminalization laws do not require intent to transmit or actual HIV transmission, and they often do not reflect contemporary scientific understanding of HIV treatment and prevention. Currently, 32 states have laws that criminalize PLWH, and 28 states impose increased penalties tied to a person’s HIV status. These laws reflect and reinforce fear-based and punitive social beliefs about HIV. They frequently criminalize behaviors that pose no or negligible risk of HIV transmission (e.g., spitting or biting), and rely on outdated legal frameworks that have not kept pace with scientific evidence demonstrating that effective treatment eliminates transmission risk. Moreover, HIV criminalization laws have not been shown to improve public health outcomes.
Raising awareness and reducing stigma are two strategies that have supported successful legislative repeal or reform of laws criminalizing PLWH. As Brad Sears stated in the Advocate, “An HIV-free generation won’t happen without ending HIV stigma.” Accordingly, improving responses to the HIV epidemic requires not only expanded public health outreach and the decriminalization of PLWH, but also a clearer understanding of people’s stigmatizing beliefs and attitudes, as these contribute to the persistence of punitive HIV-related laws. In this brief, we analyze the current extent of HIV stigma in the United States and its connection to the continued criminalization of PLWH.
HIV Stigma in the United States
To understand HIV stigma in the United States, we analyzed data from the General Social Survey (GSS). The GSS is a nationally representative survey that captures U.S. adults’ attitudes on a wide range of social issues, including beliefs about PLWH.
The present analysis focuses on two distinct dimensions of HIV stigma, fear-based and blame-based stigmatizing beliefs, among adult respondents from 2021 to 2024:
- Fear-based stigma reflects respondents’ fear of being around PLWH, capturing exaggerated and inaccurate perceptions of HIV transmissibility and social avoidance. For example, a person may falsely believe that simply being in close proximity to a PLWH—such as sharing a public space or engaging in casual contact—could result in infection.
- Blame-based stigma reflects respondents’ beliefs that PLWH have engaged in immoral or blameworthy behaviors, capturing moral judgements and responsibility attribution for HIV infection. For example, someone might believe that PLWH engage in reckless behaviors and therefore deserve less sympathy, support, or access to care.
Fear-based stigma and blame-based stigma, which run counter to scientific evidence, contribute to social and political conditions, including HIV criminalization and other structural forms of discrimination.
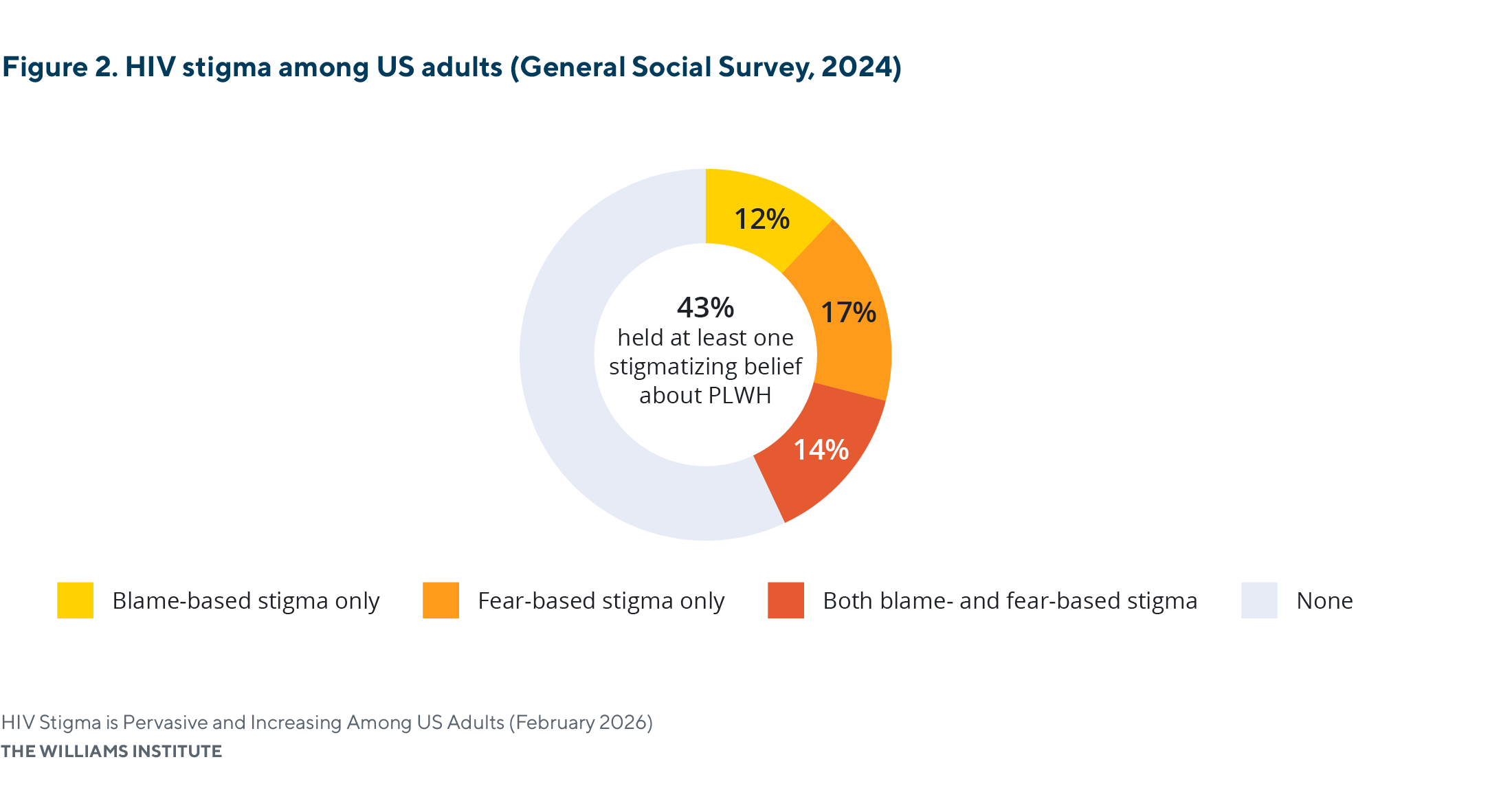
Stigmatizing beliefs about people living with HIV are common among U.S. adults.
- In 2024, more than two in five (43%) adults held at least one stigmatizing belief about PLWH.
- About one-quarter (26%) of adults believed that PLWH have engaged in immoral or blameworthy behaviors, and nearly one-third (31%) of U.S. adults reported fear of being around PLWH.
The prevalence of HIV stigma has increased in recent years.
- In 2021, 31% of adults held at least one stigmatizing belief toward PLWH; this increased to 43% in 2024.
- The share of adults who reported both fear- and blame-based stigma nearly doubled between 2021 and 2024, increasing from 8% to 14%.
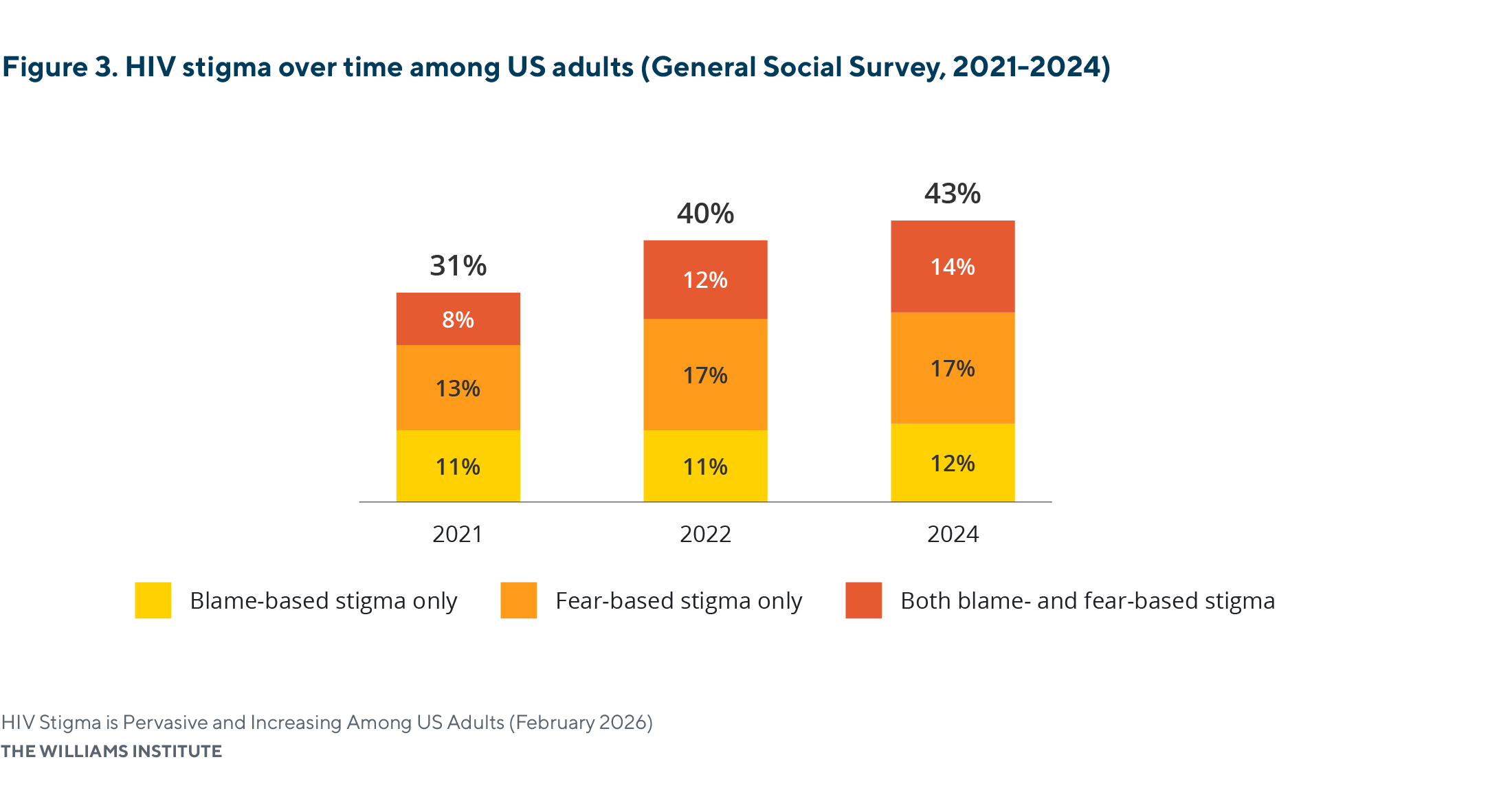
Note: Percentages may not sum exactly due to rounding. All values rounded to the tenth decimal place are reported in Appendix Table A1. Statistically significant differences in HIV stigma were observed between 2021 and 2022 and between 2021 and 2024; no statistically significant difference was observed between 2022 and 2024.
Stigmatizing beliefs about HIV are generally consistent across racial and ethnic groups.
- There were no significant differences in stigmatizing beliefs across racial groups.
- Over half of white adults (58%) and Black adults (61%) did not report any stigmatizing beliefs.
- Hispanic adults (56%) reported a higher prevalence of stigmatizing beliefs than white (42%) and Black (39%) adults; however, this difference was not statistically significant.
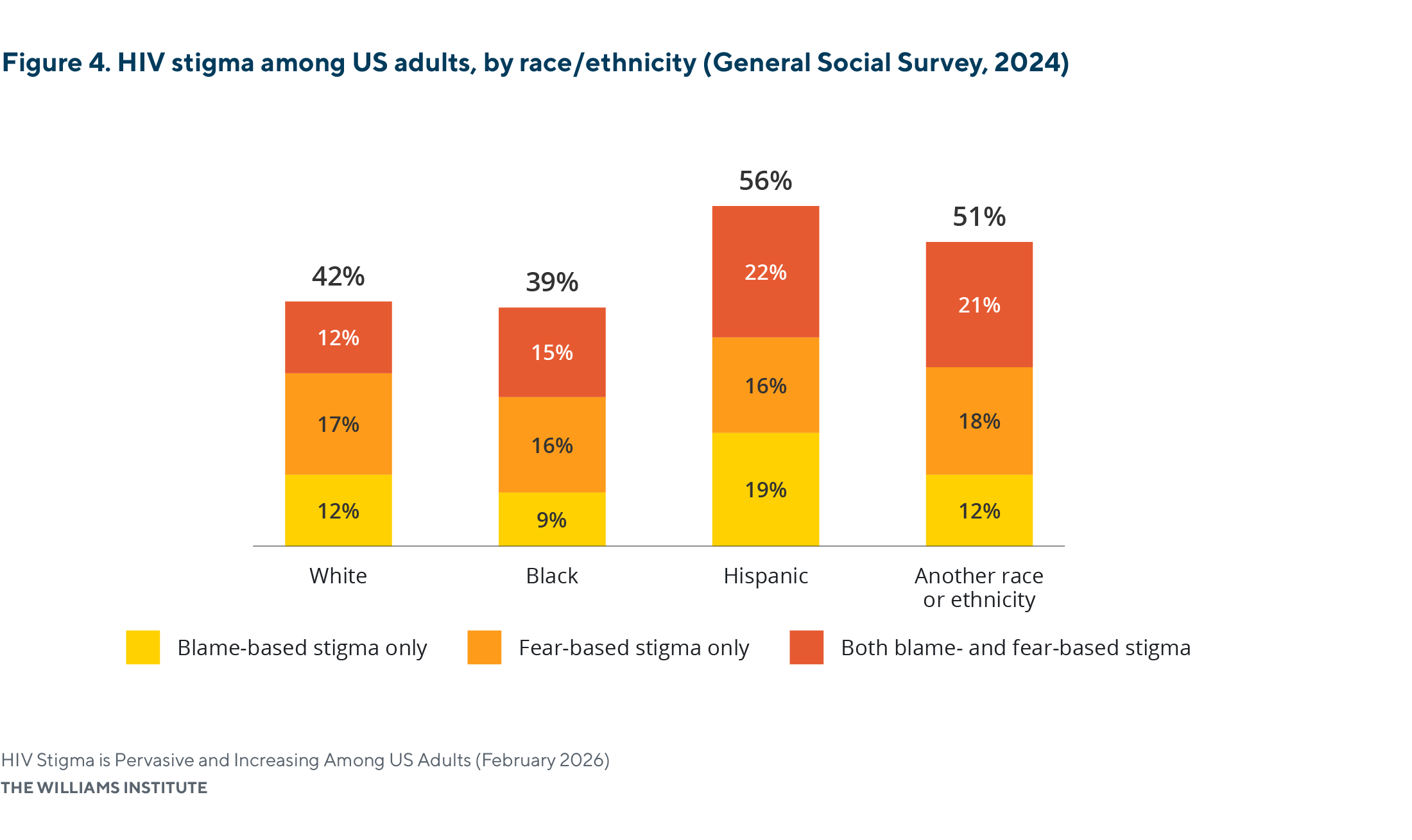
Note: Percentages may not sum exactly due to rounding. All values rounded to the tenth decimal place are reported in Appendix Table A1. Differences in HIV stigma were not statistically significant across racial and ethnic groups at the 95% confidence level.
Stigmatizing beliefs about people living with HIV are most prevalent among individuals who identify as heterosexual.
- Nearly one-half (45%) of heterosexual adults reported one or more stigmatizing beliefs about PLWH.
- In contrast, adults who identify as gay or lesbian reported the lowest prevalence of stigmatizing beliefs at 11%. No gay or lesbian respondents reported both fear-based and blame-based stigma.
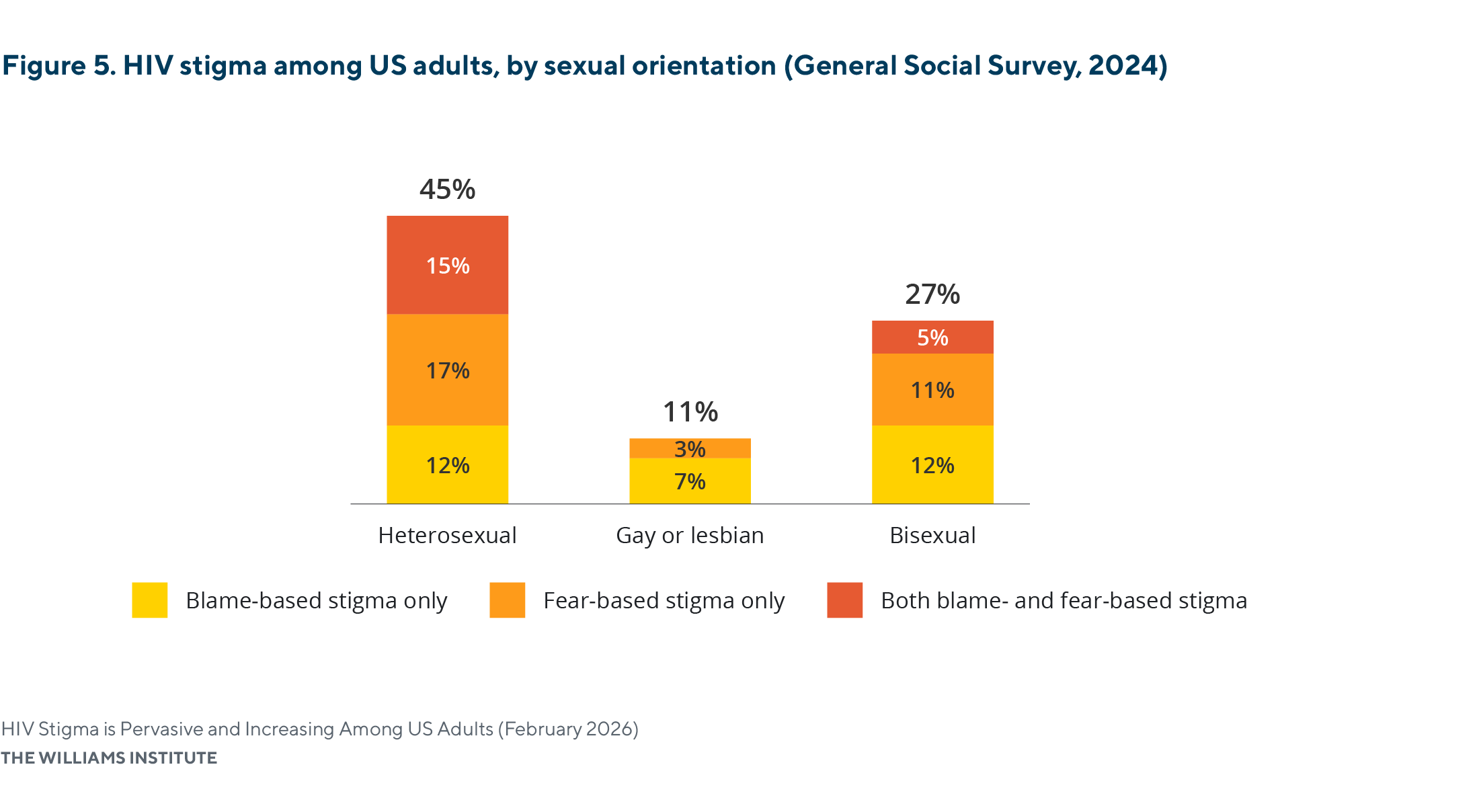
Note: Percentages may not sum exactly due to rounding. All values rounded to the tenth decimal place are reported in Appendix Table A1. Statistically significant differences in HIV stigma were observed between heterosexual and gay or lesbian respondents, but not between bisexual respondents and the other groups.
Stigmatizing beliefs generally decrease as educational attainment increases.
- About half of adults with a high school diploma (52%) or less (51%) reported at least one stigmatizing belief.
- Stigmatizing beliefs were moderately less prevalent among individuals with some college education (40%) or higher—bachelor’s (39%) and graduate degrees (37%)—compared with those with a high school degree (52%) or less (51%), though these differences were not statistically significant.
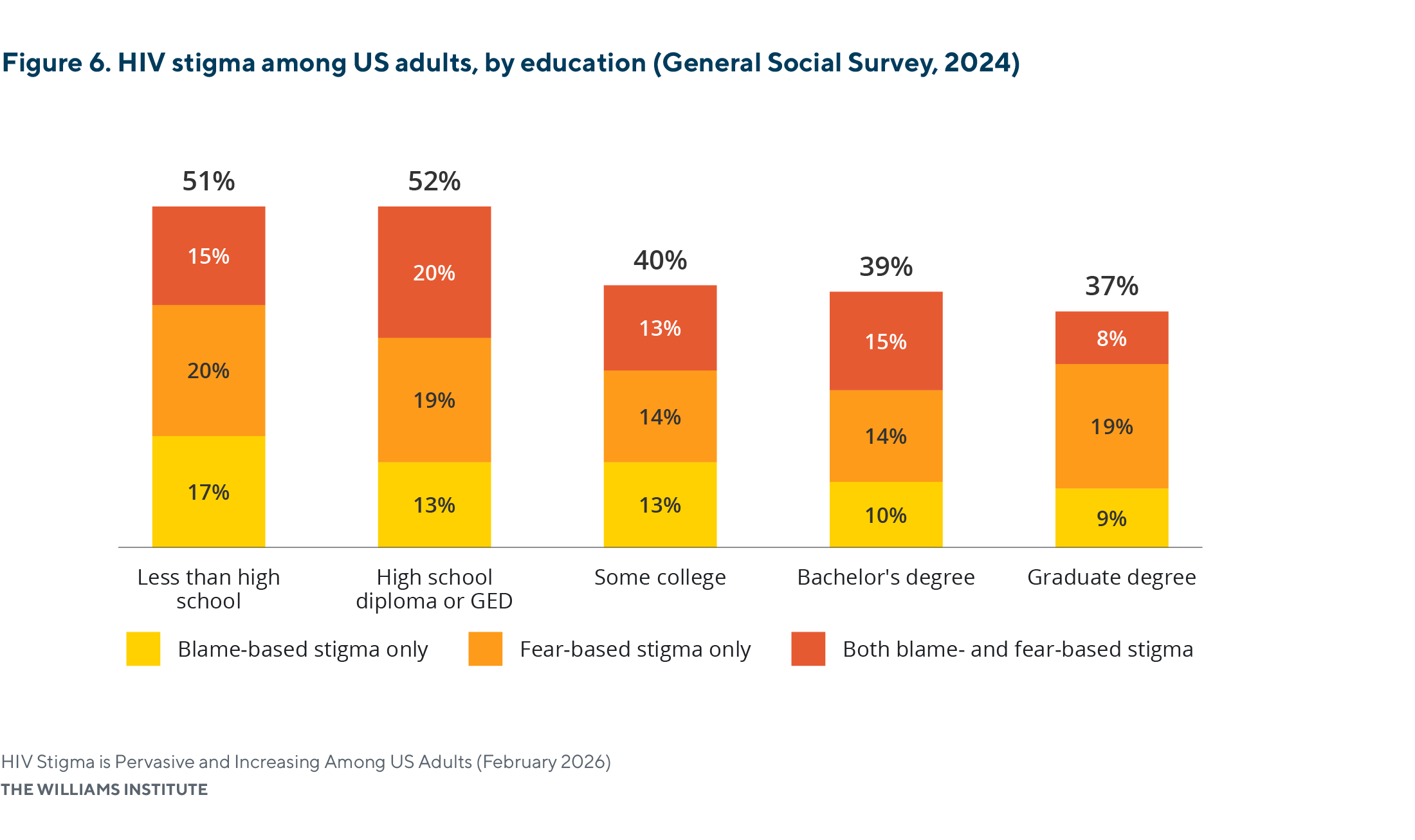
Note: Percentages may not sum exactly due to rounding. All values rounded to the tenth decimal place are reported in Appendix Table A1. No statistically significant differences in HIV stigma were observed across educational levels at the 95% confidence level.
HIV-related stigma differs by political ideology, with conservatives more likely than liberals to express stigmatizing views.
- Conservatives report the highest prevalence of HIV-related stigma, with 61% endorsing at least one stigmatizing belief, compared with 28% of liberals and 38% of moderates.
- Although fear-based stigma was common across political groups, conservatives (39%) were the most likely to hold fear-based beliefs, especially compared to liberals (22%).
- Conservatives (43%) were more than twice as likely to hold blame-based stigmatizing beliefs as liberals (12%) and moderates (21%).
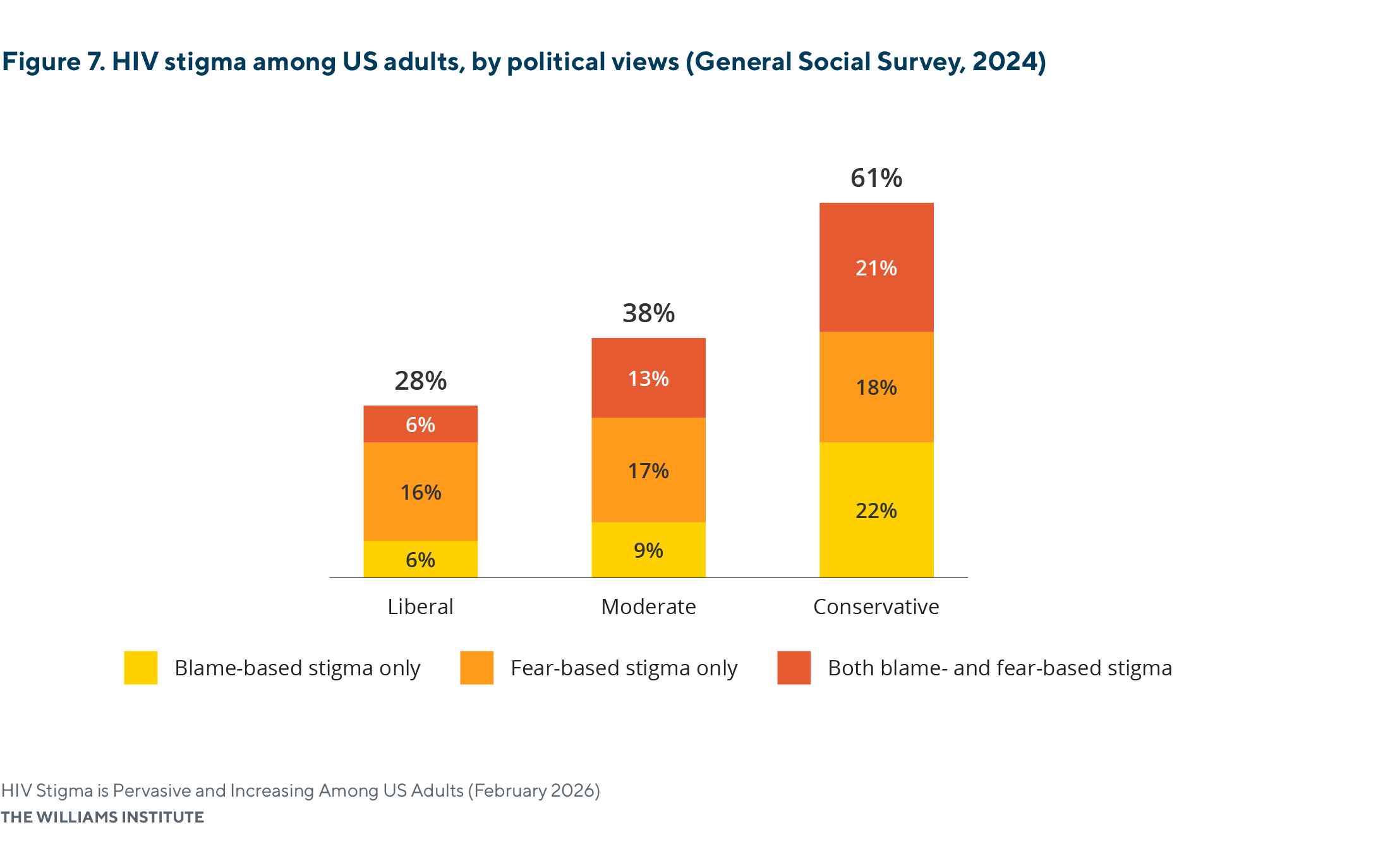
Note: Percentages may not sum exactly due to rounding. All values rounded to the tenth decimal place are reported in Appendix Table A1. Statistically significant differences in HIV stigma were observed between conservatives and the other ideological groups.
Summary of Findings on HIV Stigma in the United States
Our analysis of GSS data between 2021 and 2024 indicates that HIV-related stigma remains widespread among adults in the United States and has increased in recent years. Fear-based stigma continues to shape perceptions of HIV as a serious threat, while blame-based stigma reinforces narratives of personal responsibility and moral culpability toward PLWH. Although both forms of stigma have become more prevalent over time, fear-based stigma remains dominant across most groups. A notable exception is conservative adults, who are more likely to endorse blame-based attitudes that frame PLWH as immoral and blameworthy.
HIV Stigma and HIV Criminalization
The persistence and recent intensification of individual HIV stigma have significant implications for structural stigma, particularly in the context of HIV criminalization. Scholars have documented how HIV stigma fueled the creation of HIV-related criminal laws in the early days of the HIV epidemic in the United States. Sensationalized media coverage and political responses resulted in fear, hysteria, and misinformation about HIV, which policymakers leveraged to justify laws that disproportionately targeted LGBTQ communities. Many of these laws embody the sort of stigmatizing beliefs analyzed above.
Some laws criminalize behaviors that pose no or negligible risk of HIV transmission and thus reflect fear-based stigma toward PLWH:
- Bodily fluid exposure laws, such as Indiana’s, impose enhanced penalties on PLWH for acts such as spitting on another person, even though saliva exposure is not an HIV transmission route.
- Nondisclosure laws, enacted in several states like Florida and Ohio, criminalize PLWH for failing to disclose their HIV status prior to sexual contact, even when transmission does not or cannot occur.
Other laws reflect a moralizing form of stigma, premised on the belief that PLWH deserve punishment because they engage in behaviors deemed immoral:
- Some sex work laws, such as those in Tennessee and Pennsylvania, create increased penalties and longer prison sentences among PLWH who engage in sex work, regardless of actual transmission risk.
- Some sex offender registration laws, such as in Louisiana, mandate that PLWH who are convicted under HIV-related criminal statutes register as sex offenders, resulting in long-term legal and social consequences that extend beyond incarceration.
In practice, many HIV criminal laws reflect and drive overlapping forms of stigma, simultaneously rooted in exaggerated fears of transmission and moral judgments about the conduct of PLWH.
The Centers for Disease Control and Prevention notes that HIV-related stigma “can affect people’s health and well-being and discourage people from engaging in HIV testing, prevention, and care,” thereby increasing risk by undermining prevention, treatment, and broader public health efforts. Stigma also facilitates the enforcement of laws that criminalize PLWH solely on the basis of their medical status, often without regard for scientific advancements. As a result, responses to HIV in the United States have often been framed through punitive and moralizing terms, rather than as a treatable medical condition.
There is a broad consensus among public health experts that HIV criminalization perpetuates stigma and undermines public health objectives. By privileging punitive legal responses over evidence-based prevention and treatment, these laws discourage HIV testing and disclosure and increase social and legal risks for PLWH. In light of our findings demonstrating widespread and increasing stigmatizing beliefs, HIV criminalization both reflects and reinforces this stigma, embedding it in law in ways that continue to hinder effective public health responses.
Earnshaw, V. A., & Chaudoir, S. R. (2009). From conceptualizing to measuring HIV stigma: A review of HIV stigma mechanism measures. AIDS and Behavior, 13(6), 1160–1177; Earnshaw, V. A., Smith, L. R., Chaudoir, S. R., Amico, K. R., & Copenhaver, M. M. (2013). HIV stigma mechanisms and well-being among PLWH. AIDS and Behavior, 17(5), 1785–1795.
Centers for Disease Control and Prevention. (2024). Stigma and HIV. U.S. Department of Health and Human Services. https://www.cdc.gov/hiv/ health-equity/
Centers for Disease Control and Prevention. (2025). About HIV. U.S. Department of Health & Human Services. https://www.cdc.gov/hiv/about/index. html#cdc_disease_basics_prevention-prevention; Calabrese, S. K., Kalwicz, D. A., Zaheer, M. A., Dovidio, J. F., Garner, A., Zea, M. C., … & Eaton, L. A. (2024). The potential role of Undetectable= Untransmittable (U= U) in reducing HIV stigma among sexual minority men in the US. AIDS and Behavior, 28(2), 741-757; Huff, J. R., & Kahn, J. (2001). Discovery and clinical development of HIV-1 protease inhibitors. In Advances in Protein Chemistry (Vol. 56, pp. 213–251). Academic Press. https://doi.org/10.1016/S0065-3233(01)56007-6; Vernazza, P., Hirschel, B., Bernasconi, E., & Flepp, M. (2008). HIV-positive individuals without additional sexually transmitted diseases (STDs) and on effective antiretroviral therapy are sexually non-infectious. Bulletin des médecins suisses, 89(5).
Centers for Disease Control and Prevention. (2024). Stigma and HIV. U.S. Department of Health and Human Services. https://www.cdc.gov/hiv/health-equity/; GLAAD. (2021). 2021 State of HIV stigma study. GLAAD. Data collected from an online survey of U.S. adults. https://glaad.org/endhivstigma/2021/; GLAAD. (2022). 2022 State of HIV stigma study. GLAAD. Findings from an online survey of U.S. adults on attitudes, knowledge, and comfort with people living with HIV. https://glaad.org/endhivstigma/2022/ Pitasi, M. A., Chavez, P. R., DiNenno, E. A., Jeffries IV, W. L., Johnson, C. H., Demeke, H., … & Bradley, H. (2018). Stigmatizing attitudes toward people living with HIV among adults and adolescents in the United States. AIDS and Behavior, 22(12), 3887-3891.
Calabrese, S. K., et al. (2021). U=U awareness and HIV stigma among the general public. AIDS and Behavior, 25(10), 3213–3224; Hatzenbuehler, M. L. (2017). Structural stigma and health. The Oxford handbook of stigma, discrimination, and health, 105.
Hatzenbuehler, M. L. (2017). Structural stigma and health. The Oxford handbook of stigma, discrimination, and health, 105; Relf, M. V., Holzemer, W. L., Holt, L., Nyblade, L., & Caiola, C. E. (2021). A review of the state of the science of HIV and stigma: context, conceptualization, measurement, interventions, gaps, and future priorities. Journal of the Association of Nurses in AIDS Care, 32(3), 392-407.
Center for HIV Law and Policy. (2024). HIV criminalization in the U.S.: A sourcebook on state and federal HIV criminal law and practice. The Center for HIV Law and Policy. https://www.hivlawandpolicy.org/sites/default/files/2024-01/HIV Criminalization in the U.S. A Sourcebook on State Fed HIV Criminal Law and Practice Jan24.pdf; Galletly, C. L., & Lazzarini, Z. (2013). Criminalization of HIV transmission. Journal of the American Medical Association, 310(11), 1213–1214.
Center for HIV Law and Policy. (2025). Mapping HIV criminalization laws in the U.S. https://www.hivlawandpolicy.org/maps
Yang, Y. T., & Underhill, K. (2018). Rethinking criminalization of HIV exposure — Lessons from California’s new legislation. The New England Journal of Medicine, 378(13), 1174–1175. https://doi.org/10.1056/NEJMp1716981
Hoppe, T. (2014). Punishing disease: HIV and the criminal law. Law & Social Inquiry, 39(4), 937–965; Yang, Y. T., & Underhill, K. (2018). Rethinking criminalization of HIV exposure — Lessons from California’s new legislation. The New England Journal of Medicine, 378(13), 1174–1175. https://doi.org/10.1056/NEJMp1716981
Bernard, E. J., Symington, A., & Beaumont, S. (2022). Punishing vulnerability through HIV criminalization. American Journal of Public Health, 112(S4), S395-97. https://doi.org/10.2105/AJPH. 2022.306713; Dibble, K. E., Murray, S. M., Wiginton, J. K., Maksut, J. L., Lyons, C. E., Aggarwal, R., Augustinavicius, J. L., et al. (2022). Associations between HIV testing and multilevel stigmas among gay men and other men who have sex with men in nine urban centers across the United States. BMC Health Services Research, 22, 1179. https://doi.org/10.1186/s12913-022-08572-4; Sweeney, P., Gray, S. C., Purcell, D. W., Sewell, J., Babu, A. S., Tarver, B. A., Prejean, J., & Mermin, J. (2017). Association of HIV diagnosis rates and laws criminalizing HIV exposure in the United States. AIDS, 31(10), 1483–88. https://journals.lww.com/aidsonline/abstract/2017/06190/association_of_hiv_diagnosis_rates_and_laws.15.aspx.
Hoppe, T., & Hall, E. (2025). How Did They Do It? Analyzing the Landscape of HIV Criminalization Reform in the USA. Sexuality Research and Social Policy, 1–12.
Sears, B. (2020). An HIV-free generation won’t happen without ending HIV stigma. The Advocate. https://www.advocate.com/commentary/2020/12/01/hiv-free-generation-wont-happen-without-ending-hiv-stigma
All results, including prevalence estimates and 95% confidence intervals, are presented in the appendix (see Table A1). Findings discussed in the text are statistically significant unless otherwise noted.
The General Social Survey (GSS) is a nationally representative, probability-based survey of adults in the United States that has been conducted for more than five decades. Using a multistage, clustered sampling design, it collects information on attitudes, perceptions, behaviors, and demographic characteristics to track social trends over time. All findings we report throughout this brief were weighted to account for the GSS’s complex sampling design and to ensure national representativeness of U.S. adults; NORC at the University of Chicago. (2025). About the General Social Survey. https://gss.norc.org/about-the-gss.html
The survey is typically released in even-numbered years. However, the 2020 data were delayed due to the COVID-19 pandemic, and no data were collected in 2023 when the survey returned to its regular cycle. Accordingly, we analyze data from 2021, 2022, and 2024.
GSS survey respondents were asked to indicate their level of agreement with the following statement: “I would be afraid to be around a person with HIV because I would be worried that I could get infected.” Responses were recorded on a four-point Likert scale ranging from strongly disagree to strongly agree and were recoded for this analysis into two categories: agree and disagree.
GSS survey respondents were asked to indicate their level of agreement with the following statement: “People who have HIV have participated in immoral activities.” Responses were recorded on a four-point Likert scale ranging from strongly disagree to strongly agree and were recoded for this analysis into two categories: agree and disagree.
95% CIs: Conservatives (34, 44); Liberals (19, 31).
95% CIs: Conservatives (38, 48); Liberals (9, 15); Moderates (18; 25).
Recent research suggests that many individuals perceive HIV-related stigma to have declined in recent years; however, our findings indicate a persistent gap between public perceptions and the current reality of HIV stigma. See, GLAAD. (2024). 2024 state of HIV stigma study. https:// assets.glaad.org/m/7f1927b6af934747/original/2024-State-of-HIV-Stigma-Study.pdf?_gl=1*63cm81*_gcl_au*MjExMDgyMzg0LjE3NzA0MTE4NjI.*_ ga*MTYwODYyMDMyNS4xNzcwNDExODYy*_ga_H1BN7R59Z7*czE3NzA0MTU2NzEkbzIkZzEkdDE3NzA0MTU2NzgkajUzJGwwJGgw
Hoppe, T. (2018). Punishing disease: HIV and the criminalization of sickness. University of California Press.
Alvear, M. (n.d.). History of HIV/AIDS: 1981-1989—AIDS 1980-1984. 100Footer. https://www.100footer.net/history-of-hiv/aids-1980-1984
Cisneros, N., Foote, C., Grasso, J., Schlebecker, P., & Sears, B. (2025). Enforcement of HIV criminalization in Indiana: Body fluid/waste enhancement laws. The Williams Institute, UCLA School of Law. https://williamsinstitute.law.ucla.edu/wp-content/uploads/HIV-Criminalization-IN-Fluids-Jan-2025.pdf.
Cisneros, N., Sears, B., & Tentindo, W. (2024). Enforcement of HIV criminalization in Ohio: Analysis of criminal incidents from 2000 to 2022. The Williams Institute, UCLA School of Law. https://williamsinstitute.law.ucla.edu/wp-content/uploads/HIV-Criminalization-OH-Feb-2024.pdf; Hasenbush, A. (2018). HIV criminalization in Florida: Penal implications for people living with HIV/AIDS. The Williams Institute, UCLA School of Law. https://williamsinstitute.law.ucla.edu/wp-content/uploads/HIV-Criminalization-FL-Oct-2018.pdf.
Cisneros, N., Sears, B., & Lennon-Dearing, R. (2022). Enforcement of HIV criminalization in Tennessee. The Williams Institute, UCLA School of Law. https://williamsinstitute.law.ucla.edu/wp-content/uploads/HIV-Criminalization-TN-Jun-2022.pdf; Grasso, J., Cisneros, N., & Tentindo, W. (2025). HIV criminalization in Pennsylvania: Enforcement of “prostitution and related offenses” crimes. The Williams Institute, UCLA School of Law. https://williamsinstitute.law.ucla.edu/wp-content/uploads/HIV-Crim-Prostitution-PA-Oct-2025.pdf
Center for HIV Law and Policy. (2024). Tennessee (in HIV criminalization in the U.S.: A sourcebook on state and federal HIV criminal law and practice). https://www.hivlawandpolicy.org/sites/default/files/2024-01/Tennessee%20-%20Pages%20from%20HIV%20Criminalization%20in%20the%20U.S.%20A%20Sourcebook%20on%20State%20Fed%20HIV%20Criminal%20Law%20and%20Practice%20Jan24-7.pdf; Cisneros, N., Sears, B., & Lennon-Dearing, R. (2022). Enforcement of HIV criminalization in Tennessee. The Williams Institute, UCLA School of Law. https://williamsinstitute.law.ucla.edu/wp-content/uploads/HIV-Criminalization-TN-Jun-2022.pdf.
Centers for Disease Control and Prevention. (2024). Stigma and HIV. U.S. Department of Health and Human Services. https://www.cdc.gov/hiv/health-equity/
Cisneros, N., Foote, C., Schlebecker, P., & Sears, B. (2024). HIV criminalization in Indiana: Evaluation of transmission risk. The Williams Institute, UCLA School of Law. https://williamsinstitute.law.ucla.edu/wp-content/uploads/HIV-Crim-Transmission-IN-Nov-2024.pdf; Hasenbush, A., & Zanoni, B. (2016, December). HIV criminalization in California: Evaluation of transmission risk. The Williams Institute, UCLA School of Law. https://williamsinstitute.law.ucla.edu/wp-content/uploads/HIV-Criminalization-Transmission-Dec-2016.pdf; Sears, B., & Goldberg, S. K. (2020, February). HIV criminalization in Florida: Evaluation of transmission risk. The Williams Institute, UCLA School of Law. https://williamsinstitute.law.ucla.edu/wp-content/uploads/HIV-Crim-Transmission-FL-Mar-2020.pdf; Sears, B., & Goldberg, S. K. (2020, February). HIV criminalization in Georgia: Evaluation of transmission risk. The Williams Institute, UCLA School of Law. https://williamsinstitute.law.ucla.edu/wp-content/uploads/HIV-Crim-Transmission-GA-Mar-2020.pdf.
Hoppe, T. (2014). From sickness to badness: The criminalization of HIV in Michigan. Social Science & Medicine, 101, 139–147. https://doi.org/10.1016/j.socscimed.2013.11.007
American Medical Association. (2019). H-20.914 Discrimination and criminalization based on HIV seropositivity. AMA PolicyFinder. https://policysearch.ama-assn.org/policyfinder/detail/HIV?uri=%2FAMADoc%2FHOD.xml-0-1254.xml; National Alliance of State and Territorial AIDS Directors. (2022). HIV decriminalization health department talking points and FAQs. https://nastad.org/sites/default/files/2022-06/PDF_HIV-Decriminalization-Health-Department-Talking-Points-and-FAQs.pdf; The White House Office of National AIDS Policy. (2021). National HIV/AIDS Strategy for the United States 2022–2025. https://files.hiv.gov/s3fs-public/NHAS-2022-2025.pdf.